
"Not only do we lose patients and we lose this opportunity to actually take good care of them, but it actually undermines their trust in us as a profession," says A. Lenore Ackerman, MD, PhD.
"Not only do we lose patients and we lose this opportunity to actually take good care of them, but it actually undermines their trust in us as a profession," says A. Lenore Ackerman, MD, PhD.

“It's pretty apparent that if physicians are not going to be reimbursed properly for telehealth, they're not going to use utilize it,” says Lisa J. Finkelstein, DO, FACOS.

“I think being savvy about how you deal with BCG supply on the administrative side is important,” says Suzanne B. Merrill, MD, FACS.

“Allowing the waiver to continue indefinitely would be a tremendous win for telehealth for both sides, the patients and the health care providers,” says Kara L. Watts, MD.
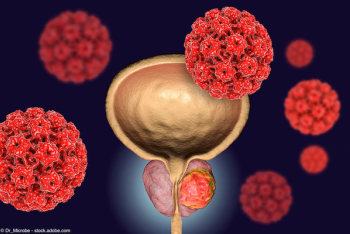
Scott T. Tagawa, MD, discusses trials exploring 177Lu-PSMA-617 in settings earlier than it’s FDA-approved indication for patients with heavily pretreated metastatic castration-resistant prostate cancer.

Melissa A. Laudano, MD, highlights 3 studies in overactive bladder/incontinence being presented at the 2023 American Urological Association Annual Meeting.

Helen L. Bernie, DO, MPH, highlights 4 studies in sexual dysfunction being presented at the 2023 American Urological Association Annual Meeting.
“In terms of next steps, we are collaborating with other institutions…to see how our model performs in their patient populations,” says Eric Li, MD.
Michael S. Cookson, MD, MMHC, highlights 5 studies in prostate cancer being presented at the 2023 American Urological Association Annual Meeting.

"In the periods where BCG utilization dropped, we saw a concomitant increase in mitomycin C," says Brian Chun, MD.

“He’s had just such a huge impact for me as a role model, a teacher, a wonderful support system, just such a kind-hearted person,” says Stacy Loeb, MD, MSc, PhD (hon).
“Waiting for others to fix health care is not a good strategy. Instead, be determined to begin your journey to your mountaintop of joy and fulfillment,” says Scott A. MacDiarmid, MD, FRCPSC.

"Even just the process of getting that β3 agonist is going to cost them time and energy and effort that can be quite frustrating and take a lot out of you," says A. Lenore Ackerman, MD, PhD.
“We were actually quite pleased with how well our model performed, particularly in the independent cohort that was separate from our training cohort,” says Eric Li, MD.

"About 30% of women screened positive, but of course when we looked at [the data] stratified by age, about 50% of women 65 years and older had a positive screen," says Steven R. Fisher, PhD, PT, GCS.
Dr Higano provides a timeline review of safety results for GnH agonists and GnRH antagonists including the recent prospective phase 3 PRONOUNCE study for prostate cancer patients with pre-existing CV disease, followed by closing thoughts on this video series.
Dr Higano explains how the use of ADT in patients with prostat ecancer may impact metabolic and cardiovascular (CV) risk factors, and shares best practices on optimizing risk assessment, mitigation, and monitoring for these factors.
A focused discussion on how ADT is used as the backbone of prostate cancer therapy across different prostate cancer risk groups and according to metastatic and castration sensitivity status.
Tia Higano, MD, FACP, provides a historical perspective on prostate cancer the use of androgen-deprivation therapy (ADT) and on prostate-specific antigen (PSA) in diagnosis and monitoring.

"We are optimistic about this study, because it has the potential not just only for vesicovaginal fistula treatment, but it can be also used in the treatment of burns for other fistula types," says Ilaha Isali, MD.

Chandler Park, MD, discusses lessons from the ARASENS and TITAN trials on the use of triplet vs doublet therapy in patients with metastatic hormone-sensitive prostate cancer.

“The first thing I'd say is that we know these devices are safe,” says Colin Goudelocke, MD.
"Our second line [for overactive bladder] is our medications. These often can be very effective for patients, but we find that they can be also extremely limited by adverse events that are associated with those medications," says A. Lenore Ackerman, MD, PhD.
“I think clinicians can really take away that we have more work to be done in this space of evaluating patients with microhematuria, specifically when it comes to looking at assessments of upper tract urothelial carcinoma or renal cell carcinoma,” says Jacob Taylor, MD, MPH.

“We want to minimize our negative biopsies and diagnosis of grade group 1 cancers,” says Rashid Siddiqui, MD.

“I would say that these conditions are highly heterogeneous, and we've identified a number of factors that relate to different ways that the disease progresses and different ways that patients feel about the progression of their disease,” says Alisa J. Stephens-Shields, PhD.

“We might find that there's a certain type of patient that really thrives on interacting with the device and playing an active role in his or her therapy,” says Colin Goudelocke, MD.
“What we need now are biomarkers to know if the medication is going to work or not,” says Park.

"Understanding work productivity and activity impairment in the context of the treatment decisions are vital, not just for the provider who has to counsel on treatment benefits and risks, but also to the patient who's making the ultimate decision," says Angela Smith, MD, MS.