


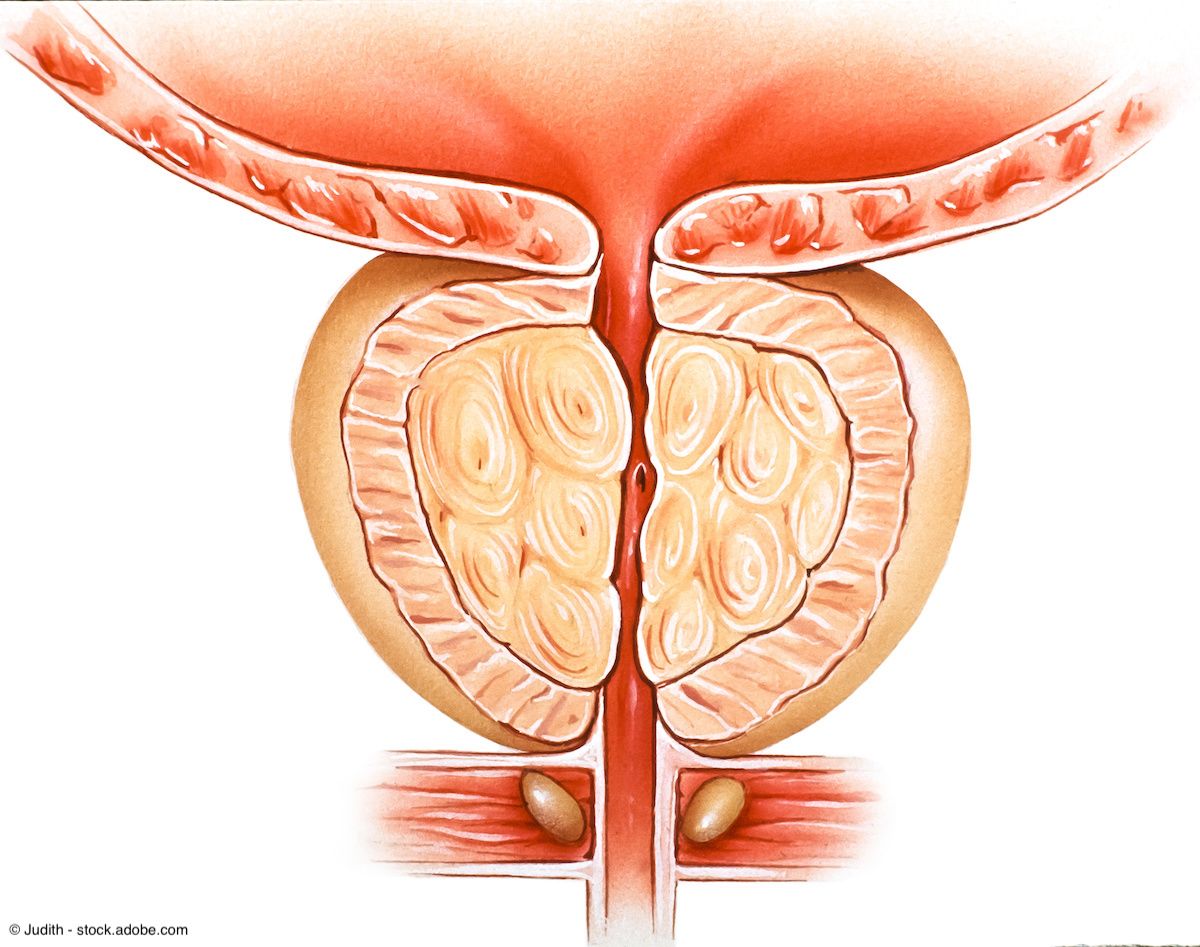

Benign Prostatic Hyperplasia
Latest News
Advertisement
Latest Videos



CME Content








Advertisement
More News

"With Aquablation, because of the real-time ultrasound image and the 3D animation that's created, you can see the actual dimensions and shape of the tunnel that's created before you even start the procedure," says Ravi Munver, MD.

"Aquablation can be used for small, medium, large, and extra-large prostates," says Ravi Munver, MD.

"Aquablation is like no other transurethral therapy that has come about in the last 100 years," says Ravi Munver, MD.

“So, we have all of this new technology that's about a year old, making surgery a lot safer for patients, making things more efficient, and [giving us] the ability to see stone removal happening from a perspective where we can visualize stone clearance in a way that we haven't been able to before,” says Marcelino E. Rivera, MD.

“While there are other treatment options available for treating BPH, there remains a significant need for much less invasive treatment approaches that can preserve and protect the integrity of the urethra and other critical structures," says Ryan Rhodes.

"[Aquablation] is the only therapy that offers the benefits of a true resective therapy, which is what it is, as well as a non-resective therapy," says Ravi Munver, MD.

"Aquablation is versatile. It can manage a very wide range of prostate sizes and shapes," says Stephen Overholser, MD.

“If you haven't used HYDROS before, or if you're concerned about doing bigger glands or tackling more difficult cases, I think we've shown in our first 35-40,000 cases that Aquablation, the therapy, is a valid therapy,” says Lewis S. Kriteman, MD, FACS.

"The evolution is continuing, now with a decade of human use of Aquablation, we can now take this to a same-day procedure––discharge the same calendar day," says Kevin C. Zorn, MD, FRCSC, FACS.

"I think it's going to help younger or less experienced urologists get more proficient at this procedure faster. That's where the AI is going to come into play," says Lewis S. Kriteman, MD, FACS.

“The technology is there, the experience is there now, and it's bringing it all together to lead to better outcomes [and a] shorter hospital stay,” says Kevin C. Zorn, MD, FRCSC, FACS.

A full market release of the HYDROS System is expected within the current quarter.

“I think particularly as we've had the technology for longer and we've used it more and become more comfortable with it, there's really nobody, necessarily, that can't be considered for it,” says Aaron M. Bernie, MD, MPH.

The guideline includes 38 recommendations on managing incontinence following treatment for localized prostate cancer or benign prostatic hyperplasia.


"The first part is how much [are patients] bothered by the symptoms?" says Akhil Das, MD, FACS.

"I'd be curious to see a validated study on whether prostate sizes have increased over time. I suspect the answer will be yes," says Joseph Song, MD.

“We've been developing different techniques in HoLEP, but there is a steep learning curve,” says Akhil Das, MD.

The new Category I code will become effective on January 1, 2026.

"From a learning curve standpoint, there's not much to learn. It tends to be fairly quick in terms of your ability to do the procedure," says Matthew E. Sterling, MD.
“Our results demonstrated that treatment with [the] Optilume BPH procedure resulted in significant symptom relief while still preserving erectile and ejaculatory function,” said Olivia Copelan, MD.

"The results showed the contemporary Aquablation procedural safety in Japanese men is exceptional in a broad range of prostate sizes along with significant symptom reduction," says Nobuyuki Hinata, MD.

"Within this paper, we discussed the importance of conservative management and lifestyle modifications as initial steps in managing BPH," says Eiftu S. Haile, MD.

In this final iteration of a 3-part series, Shawn H. Marhamati, MD, MS, shares initial insights into benefits of Aquablation in an ASC environment.
Advertisement
Advertisement
Trending on Urology Times
1
FDA approves lutetium Lu 177 vipivotide tetraxetan for PSMA-positive mHSPC
2
Individualizing androgen pathway therapy in mCSPC
3
Testosterone deficiency: FAQs from the AUA guideline
4
Large registry study reports durable 10-year outcomes with focal therapy for prostate cancer
5